
The root cause analysis (RCA) has increased in relevance over the years for proper quality management. Its implementation has grown throughout the industrial zone, including the medical field, transportation, aviation and other areas. Discover RCA’s history and its different models in this post.
Defining a RCA
A root cause analysis is a method for assessing problems based on their root causes. It analyzes the underlying factors in any given
adverse reaction to identify a problem’s source and take corrective measures to fix it. This process is unique as it delves deeper to find answers based on hidden causes and their effects, rather than merely looking at the most apparent.
Some Basic Facts
-
The RCA has been called a reactive process, meaning it’s performed after the adverse event occurs.
-
Once RCA is applied thoroughly, it soon takes the shape of a highly valuable source by becoming a proactive mechanism as it predicts problems before they occur.
Advertisement -
Although identifying root causes in a given situation forms the most important aspect of solving the problem, these causes are only secondary to the solutions sought to prevent such an occurrence in the future.
For an introduction on how to successfully implement RCA, the end of this post offers a brief summary about its process. Also included is a downloadable file of these steps for you to print and use for easy reference. Now, let’s look at the origin and history of the root cause analysis.
First Appearance of RCA in Engineering
Before its current form as a widely used process throughout all industries, RCA’s first appearance was in the field of engineering . The method is credited to none other than the founder of Toyota Industries Co., Ltd., Sakichi Toyoda.

Sakichi Toyoda
Sakichi Toyoda has been called the “King of Japanese Inventors” and the “Japanese Thomas Edison.” These titles are only suitable for a revolutionary personality, and Sakichi Toyoda’s numerous inventions speak volumes about his contributions. One of these contributions was identifying root causes to problems to solve or prevent detrimental situations. The technique Toyoda developed was called the “5 Whys.” Sakichi Toyoda is ranked number 13th on Forbes.com among the twenty most influential businessmen.
Interesting Fact: Sakichi Toyoda was also the inventor of the Jidoka principle, one of the most important industrial inventions that instantly stopped a machine when a problem occurred. He later sold Jidoka’s patent to a British firm for $150,000 and used the money to fund the start-up of Toyota, which eventually became the world’s second largest car manufacturer.
Toyota Motor Corporation First Uses RCA
The 5 Whys method developed by Toyoda was first used during the development of Toyota’s manufacturing processes in 1958. Toyota required all new employees to learn about this process as part of their initiation into the Toyota Production System.

The 5 Whys Method
The 5 Whys method is one of the earliest models used in the history of the root cause analysis, and it simply seeks to ask “why” five times until the main cause of the problem is revealed. This technique systematically rules out other causes each time a “why” is asked. For example:
Problem: The computer monitor is not working.
Why? The monitor’s light signal is not on.
Why? The monitor’s power cord is not functioning.
Why? The cord is damaged.
Why? It was placed under a heavy load.
Why? I didn’t place the cords properly when the monitor was plugged in, which caused damage.
The answer to the last why is the root cause of the initial problem of the computer monitor not working.
Although this system was praised by Toyota Production System’s initial architect, it was later criticized by Teruyuki Minoura, the managing director of global purchasing for Toyota. He called the process as too basic; lacking the proper depth and knowledge needed to find the right causes. One of the main problems identified with the method was that it was not standardized. Different employees asked new sets of “whys” each time, based on their own experiences and depth of knowledge. There was also no method of knowing if the questions asked were the correct questions to be asked in the first place. It has been revealed, however, that this issue can be offset by verifying the questions before they are asked.
RCA Schools Based on Origin
RCA evolved to accommodate many fields throughout time, and thus different approaches were eventually used in order to effectively analyze the root causes. These methods are:
- Safety-based RCA, which originated in the fields of occupational safety and health, as well as accidental analysis.
- Production-based RCA, which originated in the field of manufacturing to ensure quality control.
- Process-based RCA, which originated in the fields of business and manufacturing.
- Failure-based RCA, which originated in the fields of engineering and maintenance.
- Systems-based RCA, which originated as a combination of all of the above root cause analysis techniques, as well as borrowing concepts from risk management, systems analysis, and change management.
Six Sigma Quality
In 1986, Motorola developed a new strategy for risk management called Six Sigma. Six Sigma uses specific methods, including statistical information, to outline a RCA. It also puts its workers in a specific infrastructure based on their qualification.
The high standard of risk management achieved with Six Sigma is measured by the low number of defective products produced, which is about 99.99966% or a mere 3.4 errors or defective products per million. Due to its high success rate, the Six Sigma quality standards were soon adopted by other manufacturing industry giants, such as General Electric. Although first used in manufacturing industries, Six Sigma is now applied in service industries as well.
The Federal Aviation Administration (FAA)
The aviation industry has been actively involved in quality control, error reduction, and risk management to minimize accidents and meet FAA requirements. In 1975, FAA established the Aviation Safety Reporting System (ASRS) to conduct its safety management. Following its establishment, the FAA has reduced death rates from airline accidents by 80 percent. It has been said the success of the FAA’s risk management system comes from its separation of power; ASRS being funded by FAA, but administered by the National Aeronautics and Space Administration (NASA).
Initiation in the Health Care System
Beginning in 1999, the health care system took a special interest in root cause analysis techniques to address the high number of adverse results reported in patient safety and hospitalization standards. The statistics gathered were staggering. According the Institute of Medicine, death rates due to medical errors were estimated to be between 44,000 and 98,000 - more than the death rates of breast cancer, motor vehicle accidents, and AIDS. Death from medical errors was the eighth leading cause of death in America.
A systematic system was desperately needed as the medical field became increasingly complex, resulting in greater chances for preventable errors to
occur. The Institute of Medicine describes this need in To Err is Human, Building a Safer Health System: “Human beings, in all lines of work, make errors. Errors can be prevented by designing systems that make it hard for people to do the wrong thing and easy for people to do the right thing. Cars are designed so that drivers cannot start them while in reverse because that prevents accidents. Work schedules for pilots are designed so they don’t fly too many consecutive hours without rest because alertness and performance are compromised. In health care, building a safer system means designing processes of care to ensure that patients are safe from accidental injury. When agreement has been reached to pursue a course of medical treatment, patients should have the assurance that it will proceed correctly and safely so they have the best chance possible of achieving the desired outcome.”
Following this assessment, the root cause analysis became the preferred mechanism in health care risk management . It was also required as part of the assessment standards by The Joint Commission (TJC), one of the major accreditation bodies of health care systems in the U.S. This allowed for increased use and influence of RCA in the medical industry.
Techniques RCA Adopted or Developed
Identifying the root cause of a problem can be done in a number of different ways. Throughout the history of root cause analysis, various techniques were developed to approach different industries. Some of these techniques include:
-
Bayesian Inference - Used to determine the probability of a hypothesis through statistical inference.
-
Failure Mode and Effects Analysis - A method of studying failure and its effects to successfully weed out problem areas with minimum effort.
-
Fault Tree Analysis - Used in safety and reliability engineering fields.
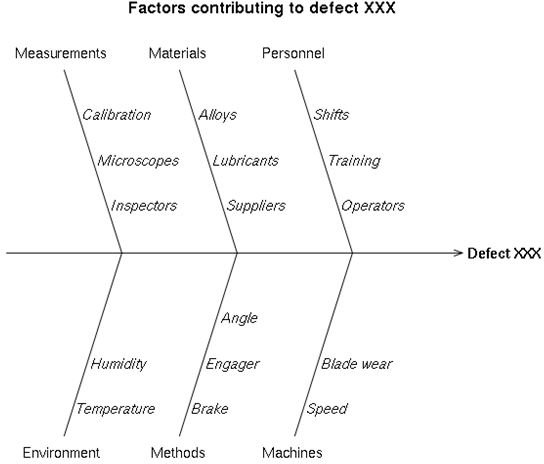
-
Ishikawa Diagram - Used in project management.
-
Pareto Analysis (80/20 Rule) - Most problems or 80 percent of the problems occur due to a few or 20 percent of the causes and by identifying these key 20 percent of the causes, you can solve the problem.
-
Change Analysis - Analyzing differences that occurred during an event to monitor change and locate root causes.
-
Current Reality Tree - A process used to study many organizational problems at once.
-
Barrier Analysis - Process industries use this model to trace energy flows and identify the barrier in those flows.
-
RPR Problem Diagnosis - A method used in the IT field.
General RCA Corrective Action Process
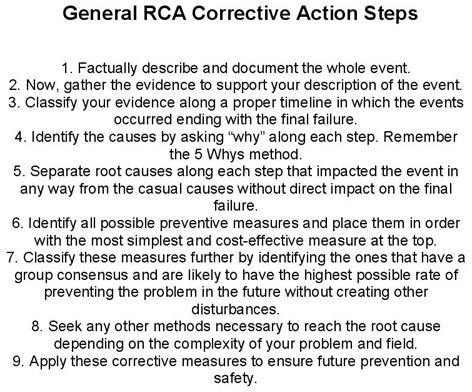
Using root cause analysis techniques successfully depends on established principles, such as proper documentation, finding lowest cost solutions, identifying more than one root cause if present, defining events and failures properly, and establishing a timeline. After establishing these principles, a step-by-step approach can be followed to effectively conduct a RCA. Below are steps that can be used to implement the RCA process. These are general rules you should modify according to your own specific field. I have also attached these steps as a downloadable file for you to print for easy reference.
1. Factually describe and document the whole event.
2. Gather the evidence to support your description of the event.
3. Classify your evidence along a proper timeline in which the events occurred ending with the final failure.
4. Identify the causes by asking “why” along each step. Remember the 5 Whys method .
5. Separate root causes along each step that impacted the event in any way from the casual causes without direct impact on the final failure.
6. Identify all possible preventive measures and place them in order with the most simplest and cost-effective measure at the top.
7. Classify these measures further by identifying the ones that have a group consensus and are likely to have the highest possible rate of preventing the problem in the future without creating other disturbances.
8. Seek any other methods necessary to reach the root cause depending on the complexity of your problem and field.
9. Apply these corrective measures to ensure future prevention and safety.
References
-
NNDB. “Sakichi Toyoda ”
Forbes.com. “Twenty Most Influential Businessmen:Sakichi Toyoda (1867-1930) ,”
Ghinassi_. Root Cause Analysis_. University of Pittsburgh, Dec., 9th, 2008. NASMHPD.
Institute of Medicine. To Err is Human: Building a Safer Health System. Washington D.C. National Academy Press, 2009.
Image Credits:
Wikimedia Commons. Sakichi Toyoda: http://en.wikipedia.org/wiki/File:Sakichi_Toyoda_new.png
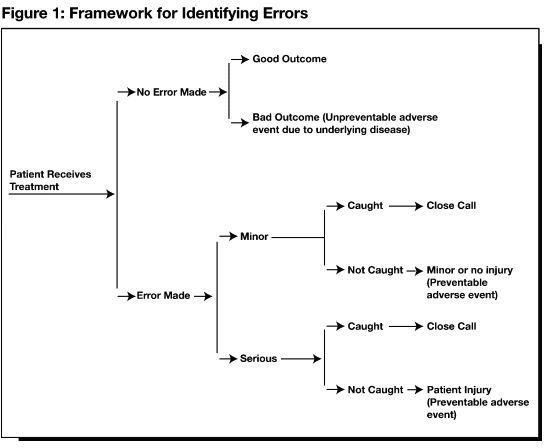
QUIC.Framework for Identifying Errors. http://www.quic.gov/Report/fig1.htm
General RCA Corrective Action Steps: Created by Hannah Grace.
Wikimedia Commons. Six Sigma. http://en.wikipedia.org/wiki/File:Six_sigma-2.svg
Wikimedia Commons. NASA Logo. http://en.wikipedia.org/wiki/File:NASA_logo.svg
Wikimedia Commons. Toyota. http://en.wikipedia.org/wiki/File:Toyota.svg


